
Depression does not simply make you sad. In many cases, it shuts off the ability to feel pleasure entirely, and that is a different problem with a different mechanism. Anhedonia, the clinical term for this loss, is not a symptom you can talk yourself out of. It reflects measurable changes in the brain’s reward circuitry, and understanding those changes tells you a lot about why certain treatments work while others fall flat.
Loss of Capacity vs. Loss of Motivation: Why the Difference Matters
Most people assume anhedonia means “not enjoying things anymore,” but that framing collapses two separate problems into one. Researchers now distinguish between the inability to experience pleasure when it arrives and the inability to want or pursue pleasure in the first place. You can lose both, or just one.
A person who feels no pull toward activities they once loved but still reports some enjoyment when engaged in them has a motivation deficit. A person who participates but feels nothing has a hedonic capacity deficit. These map to different neural systems and respond to different interventions. Getting the distinction right matters practically: it tells a prescribing psychiatrist whether to target the wanting circuit, the feeling circuit, or both. A 2021 review in Translational Psychiatry confirmed that these two subtypes show distinct symptom trajectories and treatment response profiles (Husain & Roiser, PMID: 33536408).
Anticipatory vs. Consummatory Anhedonia: The Wanting System and the Liking System
Kent Berridge’s neuroscience research established a now-foundational distinction: wanting and liking are separate systems. Dopamine drives the wanting side, sometimes called anticipatory pleasure. Opioid peptides in the brain drive the liking side, the consummatory experience of pleasure in the moment.
In depression, the wanting system is typically hit harder first. You lose the forward pull toward rewarding experiences before you lose the capacity to feel them. This is why someone with depression can describe food as tasting normal but feel zero desire to cook a meal. The signal that normally says “this will be worth it” goes quiet. When anticipatory anhedonia is severe, consummatory anhedonia usually follows, because the brain never gets the practice of reward it needs to stay calibrated. The two deficits reinforce each other across weeks and months of untreated illness.
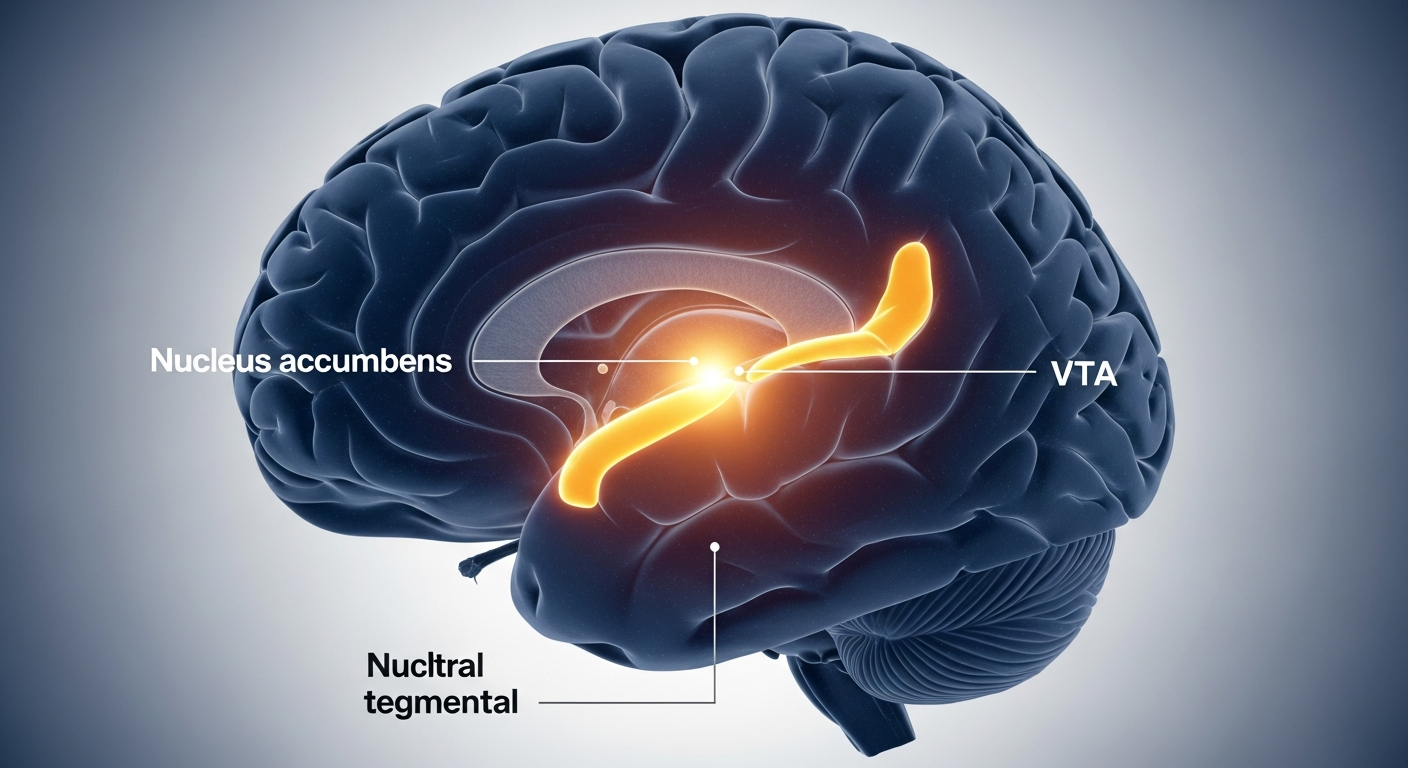
The Neural Circuit: VTA, Nucleus Accumbens, and Broken Reward Prediction
The core pathway runs from the ventral tegmental area in the midbrain to the nucleus accumbens in the forebrain. This mesolimbic tract releases dopamine in response to rewarding stimuli and, critically, in response to the anticipation of reward. Under healthy conditions, the circuit generates what neuroscientists call a reward prediction error: a signal fired when outcomes are better or worse than expected. That signal is how motivation self-calibrates.
In clinical depression, firing rates in this pathway drop. The reward prediction error signal is blunted. Studies using fMRI confirm reduced nucleus accumbens activation during reward anticipation tasks in patients with major depressive disorder (Pizzagalli et al., 2009, NIMH-funded data, PMID: 19015197). The brain stops updating its internal model of “this is worth pursuing.” Practically, that means even genuinely positive events fail to land. The circuitry is not broken, but its sensitivity is suppressed to a point where normal inputs no longer register.
Why SSRIs Sometimes Make Anhedonia Worse
Selective serotonin reuptake inhibitors work well for the mood and anxiety dimensions of depression. They are less reliable for anhedonia, and in some patients, they actively worsen it. The mechanism is indirect: serotonin pathways project onto dopamine neurons, and increased serotonergic tone can suppress dopamine output through inhibitory interneurons in the ventral striatum.
This produces what clinicians now call emotional blunting, a flattening of both negative and positive emotional responses. Patients describe it as feeling “wrapped in cotton wool.” Estimates suggest 40% to 60% of SSRI users experience some degree of emotional blunting, though rates vary significantly by molecule and dose. This is not a reason to avoid SSRIs universally. It is a reason to monitor for anhedonia specifically during the first months of treatment, and to consider augmentation or switching if the reward deficit deepens rather than improves. For a direct mechanistic comparison of agents, see our breakdown of Wellbutrin vs Lexapro mechanisms.
What Actually Helps: Bupropion, Exercise, and Ketamine
Bupropion targets dopamine and norepinephrine reuptake directly, bypassing the serotonin pathway entirely. That makes it a logical first-line choice when anhedonia is the dominant symptom rather than anxiety or rumination. Clinical data supports a stronger effect on reward processing compared to serotonergic agents.
Exercise works through a different route. Repeated aerobic activity increases the density of dopamine receptors in the striatum and reduces receptor tolerance, a process sometimes described as dopamine sensitization. A meta-analysis of 33 trials found moderate-to-large effect sizes for exercise on depression severity, with effects partially mediated by reward system normalization. The dose that shows consistent results is 30 to 45 minutes of moderate-intensity aerobic activity, three or more times per week.
Ketamine produces rapid-acting antidepressant effects partly through glutamate signaling and partly through downstream dopamine release in the nucleus accumbens. For patients with treatment-resistant anhedonia, IV ketamine or intranasal esketamine (Spravato) shows measurable improvements in reward anticipation within hours of infusion. If you want to understand how reward system dysfunction also drives emotional eating patterns, the link between GLP-1 drugs and emotional eating psychology covers overlapping circuitry. Behavioral activation, a structured protocol of scheduling rewarding activities before motivation returns, also shows solid evidence precisely because it reintroduces reward prediction error signaling at a behavioral level without waiting for pharmacology to work first.
Frequently Asked Questions
Is anhedonia always a sign of depression?
No. Anhedonia appears in schizophrenia, PTSD, Parkinson’s disease, substance withdrawal, and burnout states. It is a transdiagnostic symptom, not a depression-specific one. That said, it is one of the two core diagnostic criteria for major depressive disorder under DSM-5, making it particularly significant in mood disorder evaluation.
Why do antidepressants sometimes make anhedonia worse?
SSRIs increase serotonin tone, which can inhibit dopamine release via inhibitory projections to the ventral tegmental area. This suppresses the reward signal rather than restoring it. The result is emotional blunting that patients often find more distressing than baseline depression. Switching to a dopaminergic agent or reducing SSRI dose frequently resolves this.
Can exercise really restore the ability to feel pleasure?
Evidence says yes, with caveats. Exercise increases striatal dopamine receptor density and reduces receptor downregulation caused by chronic low dopamine output. Multiple RCTs show improvement in anhedonia-specific measures, not just general mood. The effect is dose-dependent and takes four to eight weeks to accumulate at clinical levels. It works best as an adjunct, not a standalone treatment for severe cases.
Does anhedonia eventually go away on its own?
Sometimes, but not reliably. Untreated depression can remit naturally, and anhedonia often resolves with it. However, anhedonia that persists into remission is a strong predictor of relapse. Research from NIMH longitudinal studies shows residual reward deficits between episodes in patients with recurrent MDD, suggesting the circuit dysfunction outlasts the active mood episode in a subset of patients.
If you suspect anhedonia is driving attentional and motivational deficits that look more like ADHD than classic depression, it is worth reading about AuDHD and the autism-ADHD overlap, where reward processing dysfunction appears in a distinct but related pattern.
This article is for informational purposes only and does not constitute medical advice. Consult a licensed healthcare provider before changing or starting any treatment.
Written by the DL Method Editorial Team. We research the mechanisms behind mental health conditions so you can have more informed conversations with your doctor.
Medically reviewed by Dr. Marcus Reid. Last reviewed: May 2026. Educational, not personalized medical advice.